

Usefulness of EOB-MRI for diagnosis of hepatic mestastases from pancreatic cancer at the time of hyperglycemia
Graduate School of Medicine, Hirosaki University
Drs. Shinya Kakehata, Sho Maruyama, Shingo Kakeda, Dept. of Radiology and Radiation Oncology
DATE : 2021
Introduction

Patient’s background
Male; 70 years old; body weight: 72 kg; pancreatic cancer and hepatic metastases diagnosed; diabetes mellitus; after surgery for ascending colon cancer
Assessment objectives
After surgery for ascending colon cancer. A pancreatic tail tumor was found by follow-up computed tomography (CT), and pancreatic cancer (adenocarcinoma) was diagnosed by endoscopic ultrasound-guided fine-needle aspiration. Metastases could not be found by dynamic CT, and hyperglycemia prevented sufficient evaluation of hepatic metastasis by FDG-PET/CT. Therefore, EOB-MRI was performed to search for hepatic metastases.
Contrast agent used
Gadoxetate disodium(Gd-EOB-DTPA) injection syringe, 0.1 mL/kg
Case explanation
EOB-MRI showed diffusion restriction in lobes on both sides of the liver, and loss of EOB uptake, and in the arterial phase it showed numerous nodules with ring-shaped or nodular dark staining, so the diagnosis made was multiple hepatic metastases. Surgery was not indicated, so chemotherapy was initiated. At the time of the cholecystectomy performed before chemotherapy, a hepatic biopsy was performed in relation to the hepatic metastasis from pancreatic cancer, and a histological diagnosis was made.
Imaging findings


A mass 27 mm in diameter showing a tendency toward internal necrosis was found in the pancreatic tail.
No hepatic metastasis was found (same cross-section as in Fig. 4).
Fig. 1. Dynamic CT equilibrium phase

Physiological accumulation in the intestine was found, but no positive accumulation suggesting distant metastasis was found.
However, due to hyperglycemia, FDG accumulation in the brain was lower than usual, and accumulation of FDG in the primary lesion and metastases was also expected to be reduced.
Fig. 2. FDG-PET MIP image

Positive accumulation, at SUVmax 4.0, was found in the pancreatic tail tumor.
Accumulation in the liver was patchy, and no positive accumulation suggesting hepatic metastasis was found.
Fig. 3. FDG-PET/CT fusion images
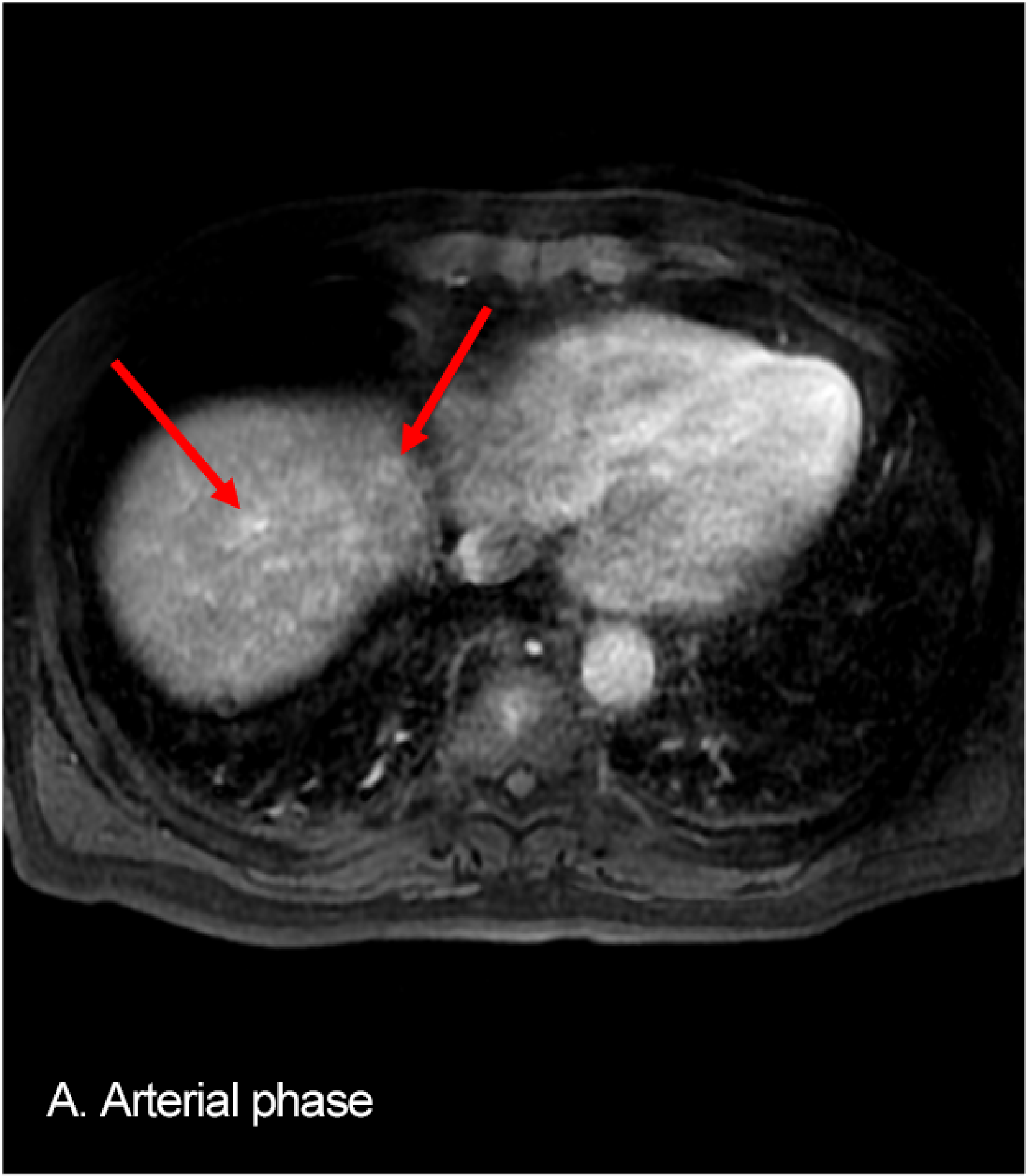



Numerous metastases were detected in both hepatic lobes. All metastases showed loss of uptake in the hepatobiliary phase, a high signal with diffusion-weighted imaging, and diffusion restriction on the ADC map, and many showed nodular dark staining in the arterial phase.
In all lesions, the internal necrosis was indistinct.
Fig. 4. EOB-MRI: A: arterial phase; B: hepatobiliary phase; C: diffusion-weighted image; D: ADC map




Fig. 5. EOB-MRI: A: arterial phase; B: hepatobiliary phase; C: diffusion-weighted image; D: ADC map
Photography protocol
| Imaging type | Photography sequence | Photography duration (min:s) | TE (msec) | TR (msec) | FA (deg) | Fat sat (type) | ETL (number) | P-MRI (Reduction Factor) | Holding breath (yes/no) |
| Dual echo | FLEX | 0:12 | 2.1/4.2 | 6.1 | 12 | DIXON | ー | ARC 2 | Yes |
| Contrast agent administration | |||||||||
| Dynamic | LAVA | 0:13 | 1.7 | 3.7 | 12 | SPECIAL | ー | ASSET 2 | Yes |
| T2WI | SSFSE | 1:00 | 80 | 2000 | 90 | ー | ー | ASSET 2 | No |
| T2WI | FSE | 2:15 | 100 | 10000 | 90 | CHESS | 24 | ARC 2 | No |
| DWI | EPI | 1:50 | 66 | 10000 | 90 | SSRF | ー | ASSET 2 | No |
| HBP | FLEX | 0:14 | 2.2/4.4 | 6.1 | 12 | DIXON | ー | ARC 2 | Yes |
| Imaging type | NEX (calculation number) | k-space | Slice thickness (mm) | FOV (mm) | Rectangular FOV(%) | Phase direction (step number) | Read direction (matrix number) | Slice Gap (mm) | Slice number |
| Dual echo | 1 | Linear | 4.8 | 380 | 80 | 160 | 320 | -2.4 | 60 |
| Contrast agent administration | |||||||||
| Dynamic | 1 | centric | 4.8 | 380 | 100 | 192 | 256 | -2 | 60 |
| T2WI | 1 | Linear | 6 | 380 | 80 | 224 | 288 | 1.2 | 20 |
| T2WI | 2 | Linear | 6 | 380 | 80 | 224 | 288 | 1.2 | 20 |
| DWI | 3 | Linear | 6 | 400 | 100 | 100 | 100 | 1.2 | 22 |
| HBP | 1 | Linear | 3.6 | 380 | 80 | 160 | 320 | -1.8 | 76 |
Devices used and contrast conditions
| MRI device | Signa HDxt 1.5T |
| Automatic injection device | Sonic Shot GX |
| Workstation | ー |
| Contrast conditions | Dose (mL) | Administration rate (mL/s) | Photography timing | |
| Gadoxetate disodium(Gd-EOB-DTPA) | 7.5 | 1 | Imaging at initiation of breath-holding, on reaching the abdominal aorta, using Smart prep | |
| Physiological saline solution for flushing | 20 | 1 |
Dynamic CT used ZIP512.
T2WI/DWI was used together with respiratory synchronization.
As the duration of breath-holding was limited to approximately 12 s, an adjustment was made.
Usefulness of Gadoxetate disodium(Gd-EOB-DTPA) contrast MRI with this patient
All hepatic metastases detected by EOB-MRI were approximately 5 mm in diameter, and the internal necrosis was indistinct, so detection by dynamic CT was difficult. As FDG-PET was performed with the patient in a hyperglycemic state, accumulation in the organs was reduced, and small hepatic metastases were difficult to detect. With pancreatic cancer, the frequency of hepatic metastasis is high, so preoperative evaluation of hepatic metastasis is important for decisions about whether surgery is indicated, and about other treatments. Although pancreatic cancer often causes abnormal glucose tolerance, EOB-MRI was shown to be useful for the decision about treatment, as there was no decrease in hepatic metastasis detection capability despite the patient being in a hyperglycemic state.
Precautions relating to administration
9. Precautions relating to patients with specific background factors (taken from the Package Insert)
9.8 Elderly patients
Administration must be performed with care, and with sufficient monitoring of the patient’s condition.
Elderly patients generally have depressed physiological function.
- *The case introduced is just one clinical case, so the results are not the same as for all cases.
- *Please refer to the Package Insert for the effects and indications, dosage and administration method, and warnings, contraindications, and other precautions with use.
