

A recurrent hepatocellular carcinoma (HCC) patient with whom arterial-phase subtraction was useful for diagnosis
Yamagata University Hospital
Dr. Yoshihiro Konno, Dept. of Diagnostic Radiology
Dr. Kazuyuki Haga, Dept. of Radiology
DATE : 2021
Introduction

Patient’s background
Female; 70s; body weight: 49 kg; recurrent hepatocellular carcinoma
Assessment objectives
During follow-up of C-type hepatic cirrhosis, arterial dark staining was found in S8 of the liver, and a mass approximately 15 mm in diameter that showed wash-out in the equilibrium phase was found there. HCC was diagnosed by biopsy, and radiofrequency ablation was then performed. Next, the repeated recurrence was treated by various percutaneous therapies and cTACE, but alpha-fetoprotein concentration increase was found.
EOB-MRI was then performed to evaluate the lesion.
Contrast agent used
Gadoxetate disodium(Gd-EOB-DTPA) injection, 0.1 mL/kg
Case explanation
A low-signal mass that was approximately 36 mm in diameter and was an elongated spheroid in shape was found in S8 of the liver in the hepatobiliary phase, and the low-signal region at the cranial end was found to have expanded in comparison with the EOB-MRI findings 9 months earlier (Fig. 1). Arterial dark staining of the cranial region of the lesion was very faint, but arterial dark staining was clear in the subtraction image, and the diagnosis made was recurrent HCC (Fig. 2). No clear arterial dark staining of the lesion caudal region was found, and this was considered to be a degenerative region associated with previous treatment. Afterwards, partial hepatectomy was performed, and the diagnosis made was moderately differentiated HCC.
Imaging findings
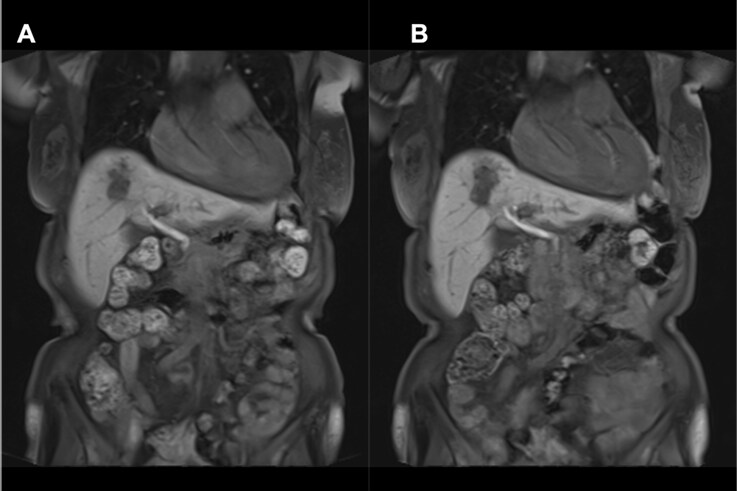
A, B) The low-signal area at the cranial end (B) has expanded in comparison with the previous image (A).
Fig. 1. Hepatobiliary phase of EOB-MRI (coronal section)
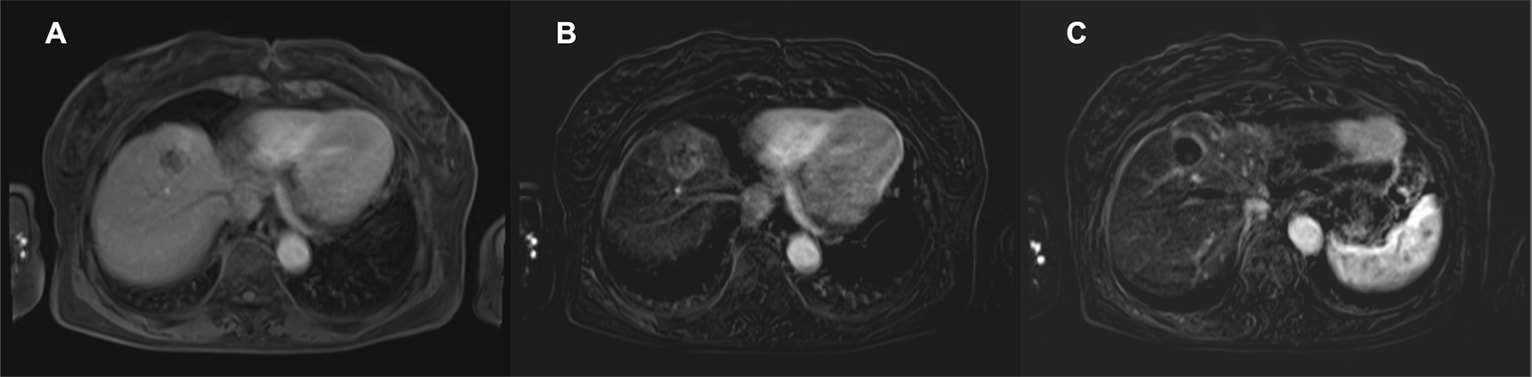
A, B) Dark staining of the liver S8 lesion cranial region (A) is clearer in the subtraction image (B).
C) Arterial-phase subtraction image: Arterial dark staining is not seen in the caudal component.
Fig. 2. EOB-MRI arterial phase
Photography protocol
| Imaging type | Photography sequence | Photography duration | TE (msec) | TR (msec) | FA (deg) | Fat sat (type) | P-MRI (Reduction Factor) |
| T2WI Cor | HASTE | 17s | 118 | 800 | 150 | (-) | GRAPPA 2 |
| T1WI Tra | 2D FLASH in-opposed phase | 20s | 1.92/4.76 | 209 | 75 | (-) | GRAPPA 2 |
| Contrast agent administration | |||||||
| Dynamic Tra | VIBE3D | 16s | 2 | 4.6 | 13 | (+) | CAIPIRINHA PE 1 / 3D 2 |
| DWI Tra | EPI (b-0,800) | *Respiratory synchronization | 72 | 2500 | 90 | (+) | GRAPPA 2 |
| T2WI Tra | TSE PACE | *Respiratory synchronization | 68 | 2000 | 160 | (-) | GRAPPA 2 |
| T2WI Tra | HASTE | 21s | 88 | 800 | 150 | (-) | GRAPPA 2 |
| Hepatobiliary phase Tra | VIBE3D | 16s | 2 | 4.6 | 13 | (+) | CAIPIRINHA PE 1 / 3D 2 |
| Hepatocyte phase COR | VIBE3D | 18s | 1.35 | 3.43 | 12 | (+) | CAIPIRINHA PE 3 / 3D 1 |
| Imaging type | Holding breath (yes/no) | NEX (calculation number) | In-plane resolution (mm) | Slice thickness (mm) | FOV (mm) | Rectangular FOV(%) | Slice Gap (mm) | Slice number |
| T2WI Cor | Yes | 1 | 320*192 | 7 | 320 | 100 | 1.5 | 20 |
| T1WI Tra | Yes | 1 | 320*192 | 7 | 320 | 81.3 | 1.5 | 24 |
| Contrast agent administration | ||||||||
| Dynamic Tra | Yes | 1 | 320*205 | 3.2 | 360 | 75 | 0 | 64 |
| DWI Tra | No | 2 | 128*96 | 7 | 320 | 75 | 1.5 | 24 |
| T2WI Tra | No | 2 | 384*230 | 7 | 320 | 81.3 | 1.5 | 24 |
| T2WI Tra | Yes | 1 | 384*250 | 7 | 320 | 81.3 | 1.5 | 24 |
| Hepatobiliary phase Tra | Yes | 1 | 320*205 | 3.2 | 360 | 75 | 0 | 64 |
| Hepatocyte phase COR | Yes | 1 | 320*224 | 4 | 400 | 100 | 0 | 52 |
* Photography duration varies between patients, due to respiratory synchronization.
Devices used and contrast conditions
| MRI device | SIEMENS MAGNETOM Aera 1.5T |
| Automatic injection device | Sonic Shot 7 (Nemoto Kyorindo Co., Ltd.) |
| Workstation | ー |
| Contrast conditions | Dose (mL) | Administration rate (mL/s) | Photography timing | |
| Gadoxetate disodium(Gd-EOB-DTPA) | 0.1ml/kg | 1.5 | Arterial phase: 30 s Portal phase: 75 s Late phase: 160 s | |
| Physiological saline solution for flushing | 50 | 1.5 |
Usefulness of Gadoxetate disodium(Gd-EOB-DTPA) contrast MRI with this patient
In addition to detection of HCC, EOB-MRI can be efficient at evaluating recurrent lesions (or similar). By means of contrast in the hepatobiliary phase, changes in the size, shape, etc., of the whole lesion can be detected readily. On the other hand, attention must be given to the contrast enhancement effects in the arterial phase being lower than with other extracellular MRI contrast media, due to the T1-shortening effect being approximately 50%1). It is possible that arterial dark staining can be found more reliably using subtraction images, as with this patient, and this is considered to be useful for improving the diagnostic capability.
References
- 1) Yasuyuki Yamashita, Tomohiro Namimoto. Gd-EOB-DTPA enhanced dynamic MR imaging: Optimization of arterial phase imaging. NICHIDOKU-IHO 55(2) 15-26.2010.
Precautions relating to administration
9. Precautions relating to patients with specific background factors (taken from the Package Insert)
9.8 Elderly patients
Administration must be performed with care, and with sufficient monitoring of the patient’s condition.
Elderly patients generally have depressed physiological function.
- *The case introduced is just one clinical case, so the results are not the same as for all cases.
- *Please refer to the Package Insert for the effects and indications, dosage and administration method, and warnings, contraindications, and other precautions with use.
