

Practical report of use for discrimination between hepatocellular carcinoma (HCC) and hemodynamic abnormalities: Discriminatory diagnosis of minute HCC versus arterioportal (AP) shunt
Graduate School of Medical Sciences, Kyushu University
Dept. of Clinical Radiology, Kyushu University Hospital: Drs. Akihiro Nishie, Tsuyoshi Tajima (current affiliation: Dept. of Diagnostic imaging and Nuclear Medicine, Tokyo Women’ s Medical University), Kousei Ishigami, Yasuhiro Ushijima (current affiliation: Dept. of Radiology, National Center for Global Health and Medicine), Daisuke Kakihara, Daisuke Okamoto (current affiliation: Dept. of Radiology, Saiseikai Fukuoka General Hospital), Hiroshi Honda
Dept. of Surgery and Science: Dr. Akinobu Taketomi
Dept. of Anatomic Pathology, Pathological Sciences: Dr. Nobuhiro Fujita
DATE : 2021
Discriminatory diagnosis of minute HCC versus AP shunt

Patient’s background and objectives of magnetic resonance imaging (MRI)
Male, 80s.
During thorough assessment of palpitations, a hepatic mass was found by chance by ultrasonography.
The patient had no medical history of chronic hepatitis. HCC was suspected, and 3 days after performing computed tomography (CT) Gadoxetate disodium(Gd-EOB-DTPA) contrast MRI was performed for the purpose of preoperative staging.
Slice section 1
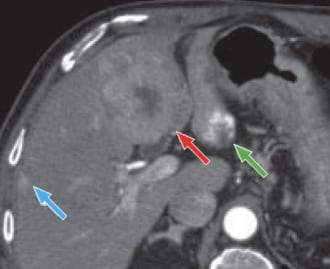
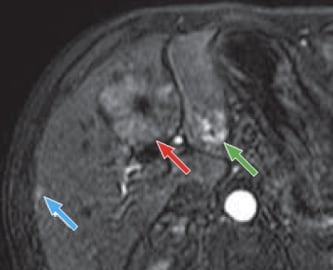
a) Arterial phase
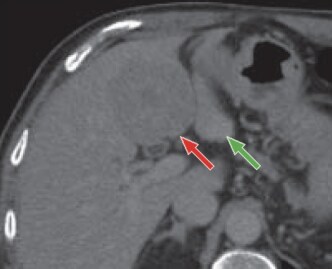
b) Late phase
Multidetector CT
In the arterial phase (a), a contrast-enhanced mass, 5 cm in diameter, was found in S4 of the liver (red arrow).
In the central part of the mass there was a low-absorption region that was suspected of having necrosis and scarring.
On the dorsal side of S3 of the liver, there was a nodule with several areas of macular contrast enhancement in the marginal region (green arrow), and below the capsule in S5 of the liver there was a small, wedge-shaped area of contrast enhancement (blue arrow).
In the late phase (b), the entire mass in S4 of the liver showed low absorption (red arrow).
On the other hand, the entire nodule on the dorsal side of S3 of the liver was visualized as a faint high-absorption region (green arrow).
The subcapsular, contrast-enhanced region in S5 of the liver showed approximately the same absorption as the hepatic parenchyma, and could not be detected.
On the basis of these findings, the mass in S4 of the liver was diagnosed as HCC (red arrow), and the nodule on the dorsal side of S3 of the liver was diagnosed as a hemangioma (green arrow). However, with respect to the subcapsular, contrast-enhanced region in S5 of the liver that was visualized in the arterial phase, it was not possible to differentiate between HCC and an AP shunt (blue arrow).
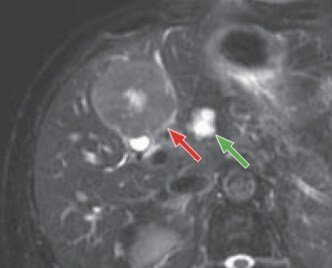
c) T2-weighted image
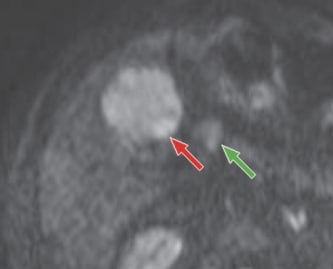
d) Diffusion-weighted image
MRI
e) Arterial phase
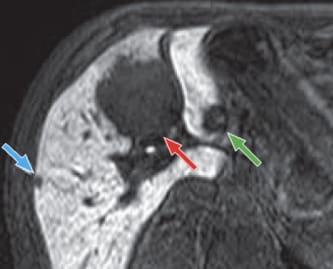
f) Hepatobiliary phase
Gadoxetate disodium(Gd-EOB-DTPA) contrast MRI
T2-weighted imaging (c) showed a mass in S4 of the liver that gave a slightly higher signal than the hepatic parenchyma (red arrow), and in the central part there was a high-signal region suggesting necrosis and scarring.
The nodule on the dorsal side of S3 of the liver showed an intense high signal (green arrow).
No clear abnormal-signal region was found below the capsule in S5 of the liver.
In diffusion-weighted imaging (d), both the mass in S4 of the liver and the nodule on the dorsal side of S3 of the liver were visualized as high-signal regions (red and green arrows).
No high-signal region was found below the capsule in S5 of the liver.
In the arterial phase (e), the mass in S4 of the liver showed contrast enhancement, except for the central region (red arrow).
Macular contrast enhancement was also found, centered in the peripheral region of the nodule on the dorsal side of S3 of the liver (green arrow). In addition, similarly to the findings with dynamic CT, a small, wedge-shaped contrast-enhanced region was found below the capsule in S5 of the liver (blue arrow).
In the hepatobiliary phase (f), both the mass in S4 of the liver and the nodule on the dorsal side of S3 of the liver were visualized as distinct low-signal regions (red and green arrows).
A small, low-signal region with a distinct boundary was also found below the capsule in S5 of the liver (blue arrow).
On the basis of these findings, similarly to the results of MDCT, the mass in S4 of the liver was diagnosed as HCC (red arrow); the nodule on the dorsal side of S3 of the liver was diagnosed as a hemangioma (green arrow); and the subcapsular, high-signal region of S5 of the liver that was visualized in the arterial phase was diagnosed as HCC (blue arrow).
Slice section 2: Section at a position further in the cranial direction than slice section 1
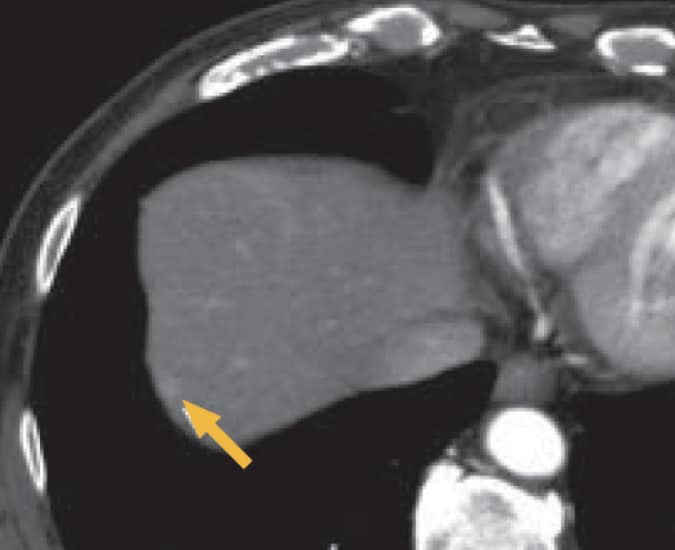
a) Arterial phase
MDCT
In the arterial phase (a), a small, nodular, early-stage dark-stained region (yellow arrow) was found in the upper right lobe, but this showed iso-absorption in the late phase (photographs not shown).
On the basis of these findings, differentiation between HCC and an AP shunt was difficult.
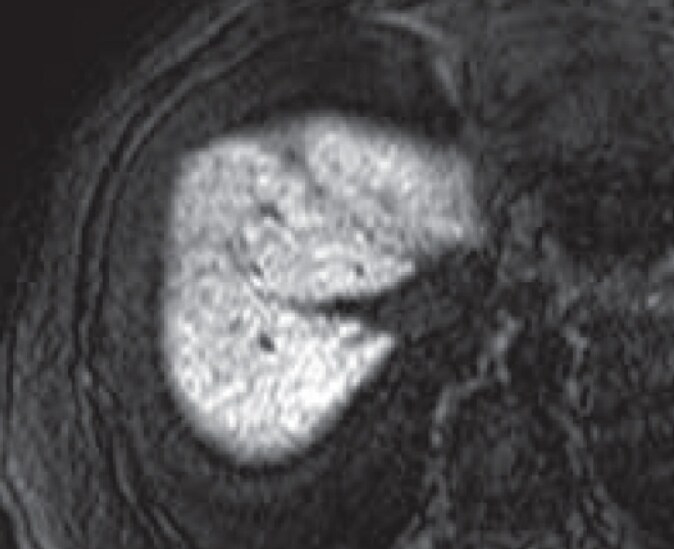
b) Hepatobiliary phase
Gadoxetate disodium(Gd-EOB-DTPA) contrast MRI
A low-signal region consistent with the small, early-stage dark-stained region found in the upper right lobe in the MDCT arterial phase (a) was not found in any of the dynamic phases, including the Gadoxetate disodium(Gd-EOB-DTPA) contrast MRI hepatobiliary phase (b). The diagnosis of AP shunt was therefore made.
Diagnostic results based on each arrow and the MRI findings
Red arrow: HCC; blue arrow: HCC; green arrow: hemangioma; yellow arrow: AP shunt
Summary
The present patient had HCC in S4 of the liver, associated with one intrahepatic metastasis below the capsule in S5 of the liver.
With this patient, the hepatobiliary phase was highly useful for qualitative evaluation of the two early-stage dark-stained regions found in the right lobe of the liver by dynamic CT.
In other words, whereas the subcapsular lesion in S5 of the liver was visualized as a distinct, nodular region with reduced Gadoxetate disodium (Gd-EOB-DTPA) uptake, and diagnosed as an intrahepatic metastasis, more Gadoxetate disodium(Gd-EOB-DTPA) uptake was found in the early-stage dark-stained region of the upper right lobe, and this was diagnosed as an AP shunt.
Indeed, the subcapsular lesion in S5 of the liver was pathologically diagnosed as HCC, and the nodule in the upper right lobe could not be located by intraoperative ultrasonography.
Gadoxetate disodium(Gd-EOB-DTPA) contrast MRI is expected to play a major role in qualitative diagnosis of small lesions that cannot readily be diagnosed by dynamic CT, and thus to contribute to selection of appropriate surgical techniques.
On the other hand, the lesion in S3 of the liver was a hemangioma.
Although diagnosis was made easily when the typical contrast pattern was shown in the arterial and portal phases after Gadoxetate disodium (Gd-EOB-DTPA) administration with the present patient, most of the lesion gave a low signal in the hepatobiliary phase, so differential diagnosis versus other tumors cannot be made on the basis of this phase alone.
Therefore, it is necessary to refer to the signal in the T2-weighted image when performing the evaluation.
Precautions relating to administration
Administration to elderly patients
Elderly patients generally show depressed physiological function, so administration must be performed with care, and with sufficient monitoring of the patient’s condition.
- * The case introduced is just one clinical case, so the results are not the same as for all cases.
- * Please refer to the Package Insert for the effects and indications, dosage and administration method, and warnings, contraindications, and other precautions with use.
