

Pre-TACE identification of visually distinguishable tumor types by Gadoxetate disodium(Gd-EOB-DTPA) contrast MRI
Kindai University Hospital
Faculty of Medicine
Dept. of Radiology
Drs. Masakatsu Tsurusaki,Takamichi Murakami
DATE : 2021
Introduction
In General Rules for the Clinical and Pathological Study of Primary Liver Cancer (edition 5), the following broad, visually distinguishable categories of hepatocellular carcinoma (HCC) tumor are defined: (i) type with indistinct margins; (ii) simple nodular type; (iii) simple nodular type with extranodular growth (iv) multinodular confluent type; and (v) infiltrative type. Leaving aside the infiltrative type, among the nodular types, HCC tumors belonging to visually distinguishable types (iii) or (iv) show high frequencies of pathological vascular invasion and intrahepatic metastasis. In addition, in patients with whom resection or liver transplantation are performed, classification as types (iii) or (iv) has been reported to be a significant factor for poor prognosis. Therefore, although systematic liver resection is the preferred treatment for these tumors, transcatheter arterial chemoembolization (TACE) is often performed with patients with whom resection is difficult. Few reports have covered the prognoses for and recurrence frequencies with TACE patients with different visually distinguishable tumor types, and the importance or impact of these types thus remains unclear. However, on the basis of their experience, the authors have the impression that, among patients with tumors of the simple nodular type with extranodular growth or the multinodular confluent type, TACE often shows low efficacy and/or is followed by early recurrence. Therefore, evaluation of the visually distinguishable tumor type before TACE is considered to be important for deciding upon the treatment procedure, including the TACE therapeutic range, drug dose, and level of embolization, whether or not radiofrequency ablation is also performed, and whether or not administration of molecular-targeted drugs (e.g. sorafenib) is initiated soon after TACE.
The present report is about the authors’ experience with a patient with HCC combining the simple nodular type and the simple nodular type with extranodular growth, with whom Gadoxetate disodium(Gd-EOB-DTPA) contrast magnetic resonance imaging (EOB-MRI) was used as preoperative diagnostic imaging at the time of TACE, for evaluation of the visually distinguishable tumor types.
Magnetic resonance imaging (MRI) method using Gadoxetate disodium(Gd-EOB-DTPA)
Sequence and sequence parameters
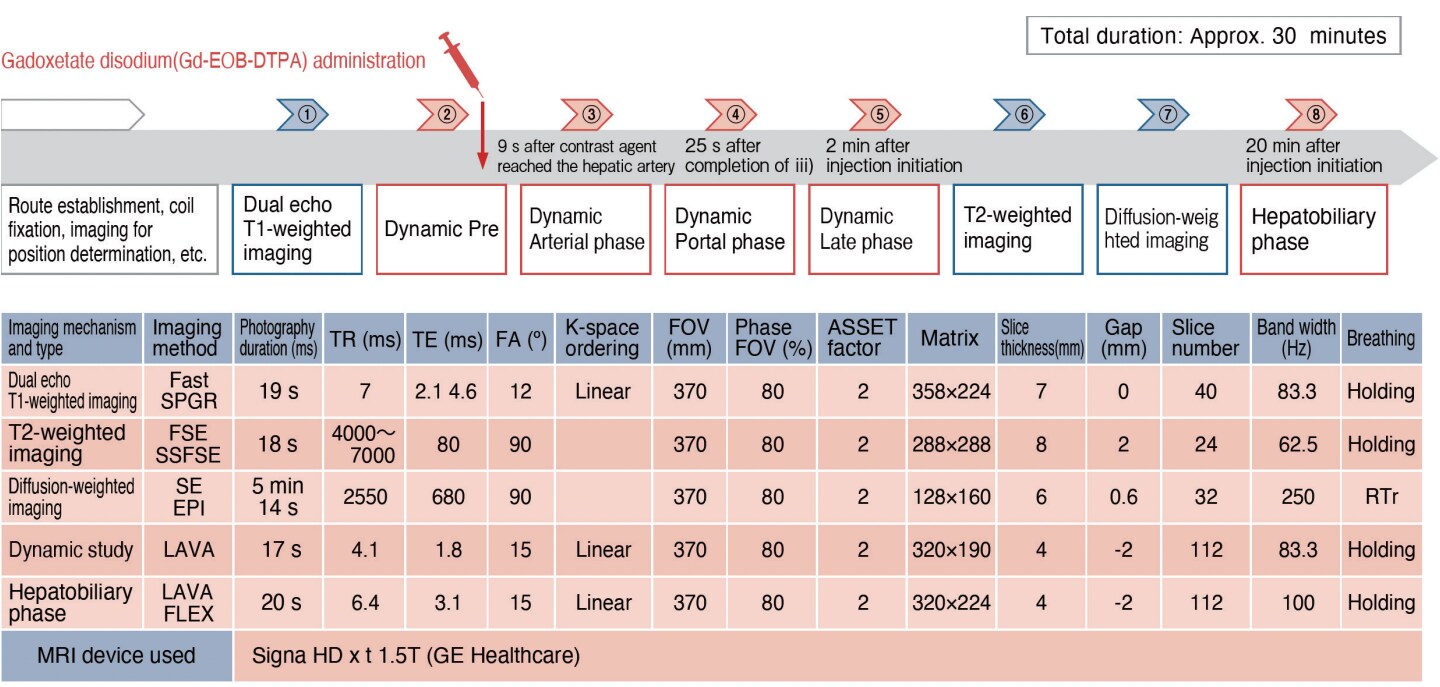
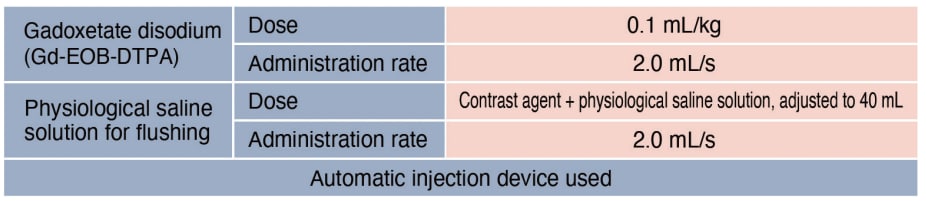
Contrast agent and administration method
Contrast Computed Tomography (CT) method

Case presentation

Patient’s background and objectives of MRI
Female, 60s.
The patient had been found to have liver disease at the age of approximately 40. Hepatic space-occupying lesions were found by ultrasonography at a medical examination, and contrast CT was performed at a local hospital in June 2012.
At that time, tumors 3 cm in diameter were found in S3 and S8 of the liver, and HCC was suspected, so the patient was referred to the authors’ hospital for thorough examination and treatment.
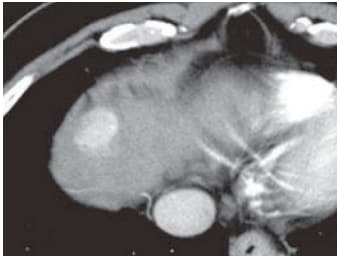
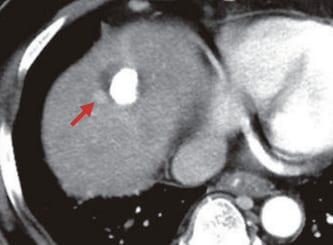
S8: Arterial phase (a)
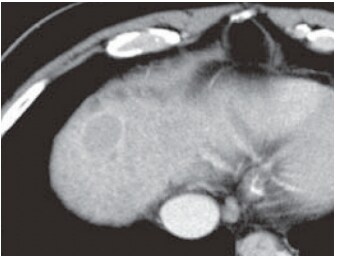
S8: Portal phase (b)
Contrast CT
CT findings
A mass 25 mm in diameter was found in S8 by dynamic contrast CT. In the arterial phase (a), it showed dark staining, and in the portal phase (b) wash-out was found in the interior of the mass, and the surrounding tissue showed capsule-like contrast enhancement.
It was considered that the mass was probably HCC with a capsule, but some of the margin was irregular, and evaluation of the visually distinguishable tumor type was difficult.
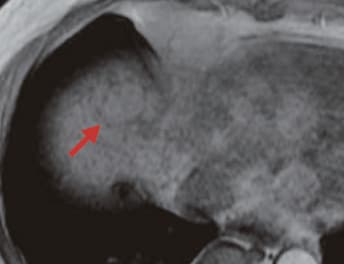
S8: T1-weighted image (c)
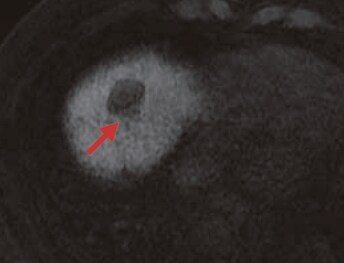
S8: Hepatobiliary phase (g)
S8: T2-weighted image (d)

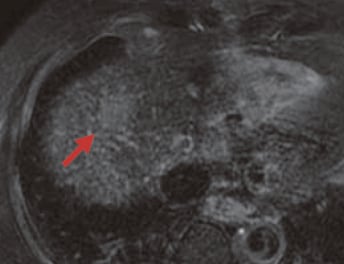
S8: Hepatobiliary phase (h)
S8: Arterial phase (e)
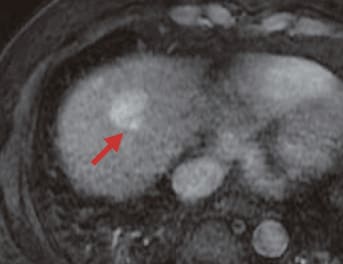
S3: Hepatobiliary phase (i)
S8: Late phase (f)
EOB-MRI images
EOB-MRI findings
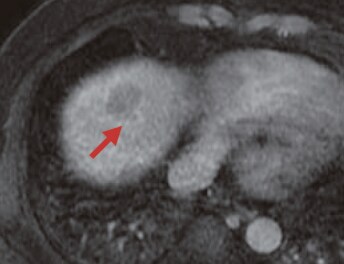
A mass 25 mm in diameter was found in S8 of the liver, showing an iso-signal or slightly high signal (arrow) with T1-weighted imaging (c), and a high signal (arrow) with T2-weighted imaging.
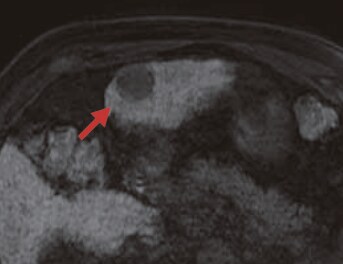
In the EOB-MRI arterial phase (e), the mass showed relatively consistently dark staining, and on the dorsal side of part of the tumor an intensely dark-stained protruding region was seen (arrow).
In the late stage (f), wash-out was found, and in the hepatobiliary phase (g) Gadoxetate disodium(Gd-EOB-DTPA) uptake was found to be absent.
The dorsal protruding locus found in the arterial phase also appeared as a region without uptake, and was therefore considered to be part of the tumor (arrow).
A coronal section (h) in the hepatobiliary phase also showed the tumor margin to be irregular (arrow), and the result of visually distinguishable tumor type evaluation was diagnosis as the simple nodular tumor type with extranodular growth and associated extracapsular infiltration.
An HCC tumor with a diameter of 30 mm was also found in S3, and in the EOB-MRI hepatobiliary phase (i) its margin was found to be circumferentially regular, so the result of visually distinguishable tumor type evaluation was diagnosis as the simple nodular type.
DSA at TACE (j)
S8: Simple CT (k) immediately after TACE
↓ 6 months later
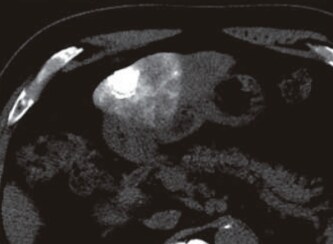
S8: Arterial phase of contrast CT (m)
S3: Simple CT (l) immediately after TACE
Course of treatment
With this patient, the presence of multiple lesions in both lobes of the liver, and the level of hepatic function together rendered surgery difficult, so TACE was performed.
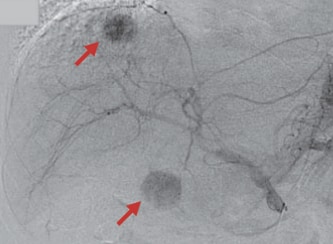
In digital subtraction angiography (j) at the time of TACE, two dark-stained loci were found inside the liver (arrows), and selective TACE was performed with each, using gelatin granules and an emulsion containing 20 mg of CDDP and 2 mL of lipiodol.
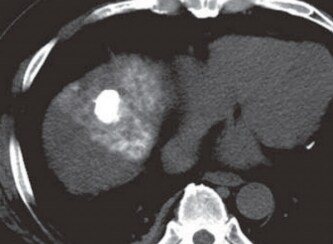
Simple CT immediately after TACE showed favorable accumulation of lipiodol in each HCC tumor (k, l).
The contrast CT arterial phase at follow-up 6 months later showed favorable accumulation of lipiodol in the HCC in S3, and no recurrence. However, dark staining was found close to the HCC in S8 that had been classed earlier as the simple nodular type with extranodular growth, suggesting localized recurrence (m; arrow).
Usefulness of EOB-MRI diagnostic results with this patient
Resection was not feasible with this patient, so pathological assessment was not performed, but pre-TACE EOB-MRI suggested a combination of two types of HCC; the simple nodular type, and the simple nodular type with extranodular growth.
Although the same procedure, selective TACE, was performed with both tumors, its effects were different; with the simple nodular type efficacy was favorable, whereas with the simple nodular type with extranodular growth localized recurrence was found relatively soon afterwards.
The present patient is considered to provide valuable information for future reference. During treatment and post-treatment follow-up, sufficient at-tention has to be given to lesions that are considered, on the basis of pre-TACE diagnostic imaging (primarily EOB-MRI), to be the simple nodular type with extranodular growth, and with some cases there may be a need for measures such as concomitant radiofrequency ablation, and/or prompt postoperative initiation of molecular-targeted agent administration.
Adverse effects (at approval)
Of the total of 1,755 subjects, 76 (4.33%) suffered adverse effects.
The principal adverse effects included the following: vasodilation (hot sensation, flushing): 16 patients (0.91%); nausea: 12 patients (0.68%); dysgeusia: 9 patients (0.51%); and headache: 8 patients (0.46%)
(total numbers in Japanese and overseas clinical studies at approval).
Precautions relating to administration
Administration to elderly patients
Elderly patients generally show depressed physiological function, so administration must be performed with care, and with sufficient monitoring of the patient’ s condition.
- *The case introduced is just one clinical case, so the results are not the same as for all cases.
- *Please refer to the Package Insert for the effects and indications, dosage and administration method, and warnings, contraindications, and other precautions with use.
