

Practical report of metastatic hepatic cancer: Diagnosis of gastric cancer hepatic metastases
Dokkyo Medical University
Dept. of Radiology:
Drs. Yasukazu Shioyama, Yasushi Kaji
Second Dept. of Surgery: Dr. Keiichi Kubota
DATE : 2021
Diagnosis of gastric cancer hepatic metastases

Patient’s background and objectives of Magnetic Resonance Imaging (MRI)
Male, 50s.
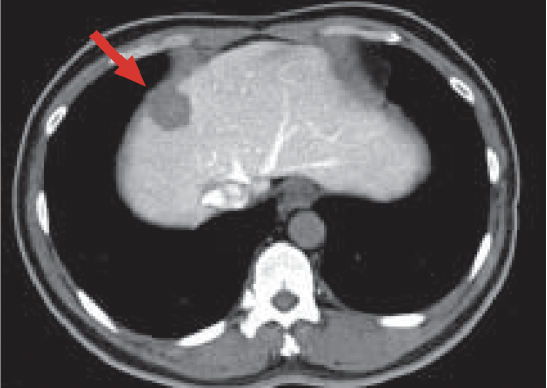
A hepatic mass was found by ultrasonography during monitoring of hepatic functional impairment at a different hospital, so the patient was referred to Dokkyo Medical University’ s Dept. of Surgery for treatment. Intravenous dynamic computed tomography (CT) had been performed at the other hospital. Although the dark staining found in the arterial phase was not very intense, this was considered to be due to dynamic CT being inappropriate, and the contrast agent dose being too low. At Dokkyo Medical University, CT during angiography was performed as a preoperative examination.
Angiography, and CT during angiography

a) Hepatic arteriography
Angiography
b) CT during arterial portography (CTAP)

c) CT during hepatic arteriography (CTHA): Phase 1

d) CTHA Phase 2
CT during angiography
Hepatic arteriography (a) showed relatively dark tumor-staining (red arrow) in S8 of the liver.
CTAP (b) showed portal blood flow to be deficient, Phase 1 (c) of CTHA showed intense dark staining throughout the liver, and Phase 2 (d) showed corona-like wash-out, so the lesion was judged to be typical hepatocellular carcinoma (HCC).
A mass showing a similar pattern was found in the margin of the lateral segment of the left lobe of the liver.
Slice section 1
e) Arterial phase
f) Portal phase
g) Late phase
h) Hepatobiliary phase
Gadoxetate disodium(Gd-EOB-DTPA) contrast
i) Diffusion-weighted imaging
MRI
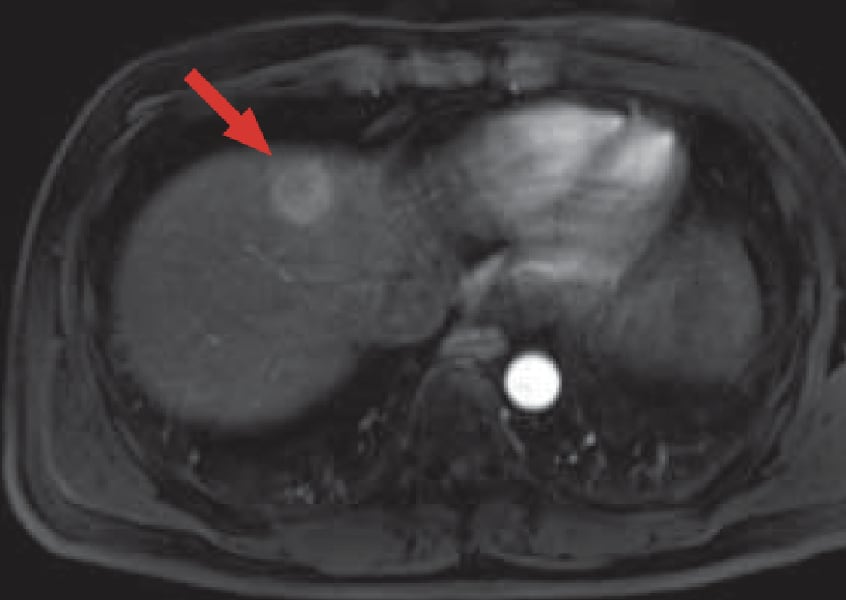
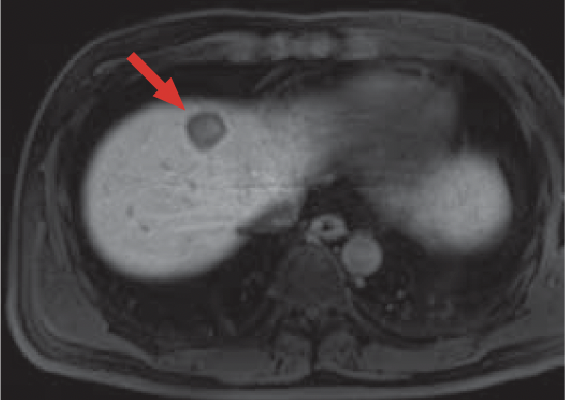
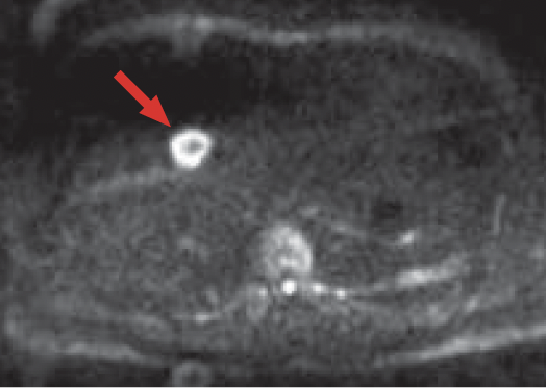
The mass shown by CT (red arrow) showed dark staining in the arterial phase (e) of Gadoxetate disodium(Gd-EOB-DTPA) contrast MRI, wash-out from the portal phase (f) to the late phase (g), and a typical HCC pattern even in the hepatobiliary phase (h).
In addition, diffusion-weighted imaging (i) showed a ring-shaped, intense, and abnormally high signal.
Slice section 2
j) Arterial phase
k) Late phase
l) Hepatobiliary phase
Gadoxetate disodium(Gd-EOB-DTPA) contrast

m) Diffusion-weighted imaging
MRI
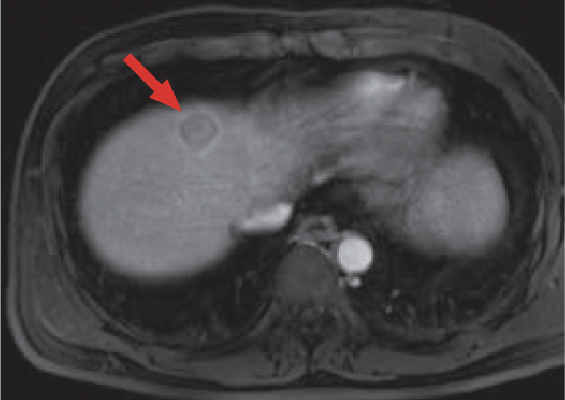
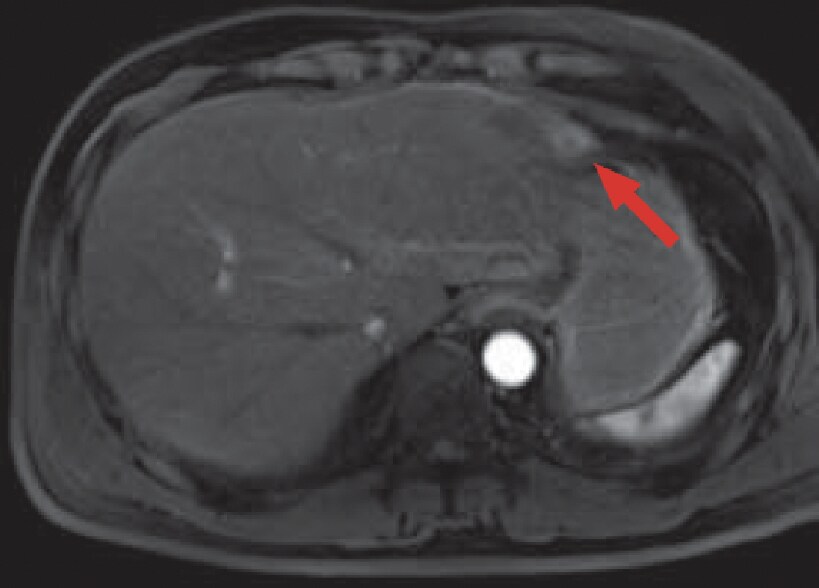
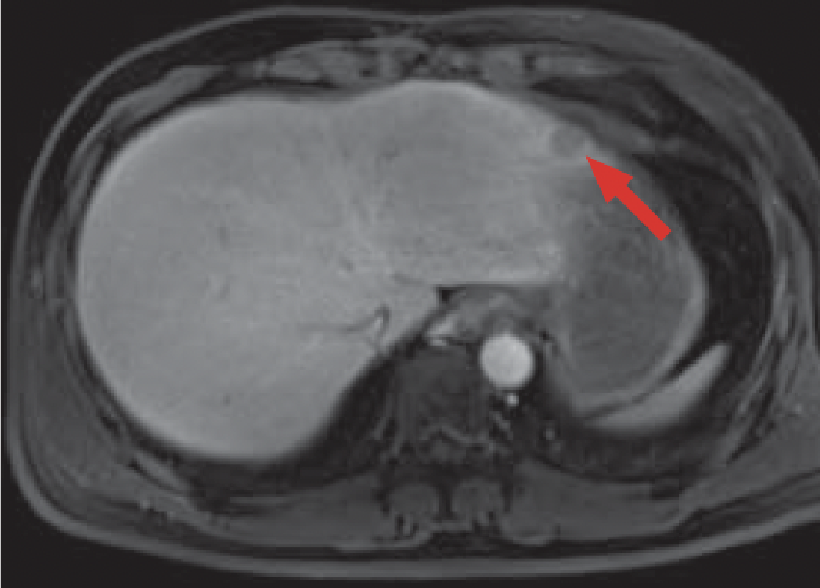
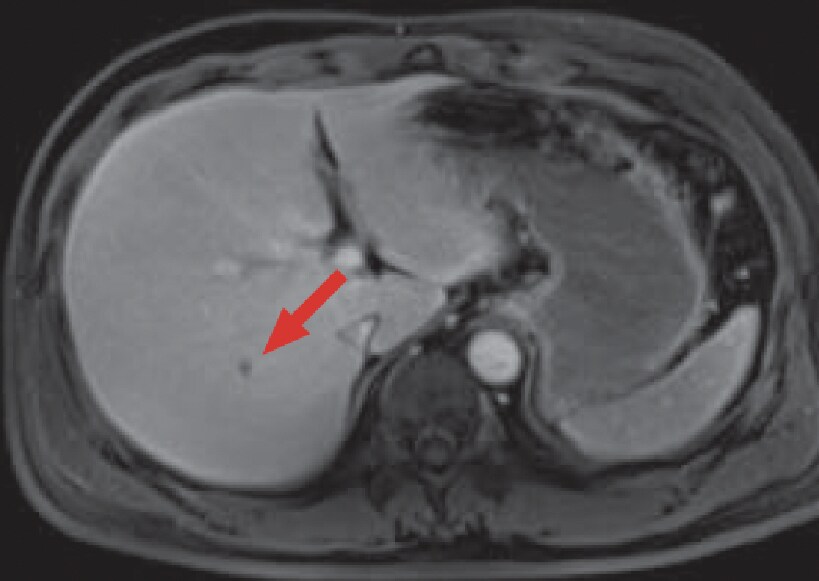
The tumor (red arrow) in the hepatic left lobe lateral segment was difficult to make out in the hepatic margin, but with diffusion-weighted imaging (m) it showed a distinct, abnormally high signal, and in the Gadoxetate disodium(Gd-EOB-DTPA) contrast MRI arterial phase (j), late phase (k), and hepatobiliary phase (l) it showed a typical image.
Slice section 3
n) Late phase
Gadoxetate disodium(Gd-EOB-DTPA)contrast

o) Diffusion-weighted imaging
MRI

p) CTHA Phase 2
CT during angiography
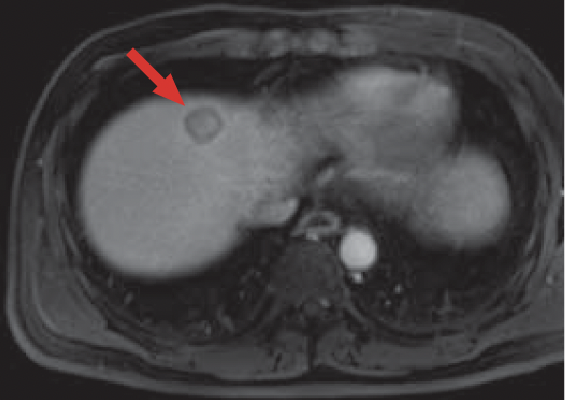
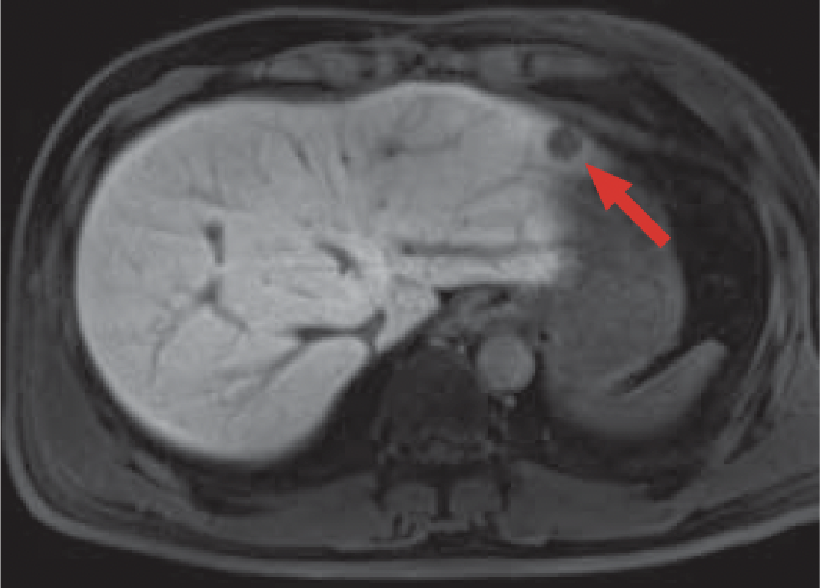
In the hepatic right lobe posterior segment, a nodule (red arrow) was found that gave a low signal in the Gadoxetate disodium(Gd-EOB-DTPA) contrast MRI late phase (n), and a high signal with diffusion-weighted imaging (o).
This nodule was difficult to distinguish from a blood vessel in CTHA Phase 1 (photographs not shown), but appeared as a dark-stained nodule in Phase 2 (p).
Reassessment of earlier findings then showed that it had also been possible to identify a point-like low-absorption region with CTAP (b).
Slice section 4
q) Diffusion-weighted imaging
MRI
r) Equilibrium phase
Contrast CT
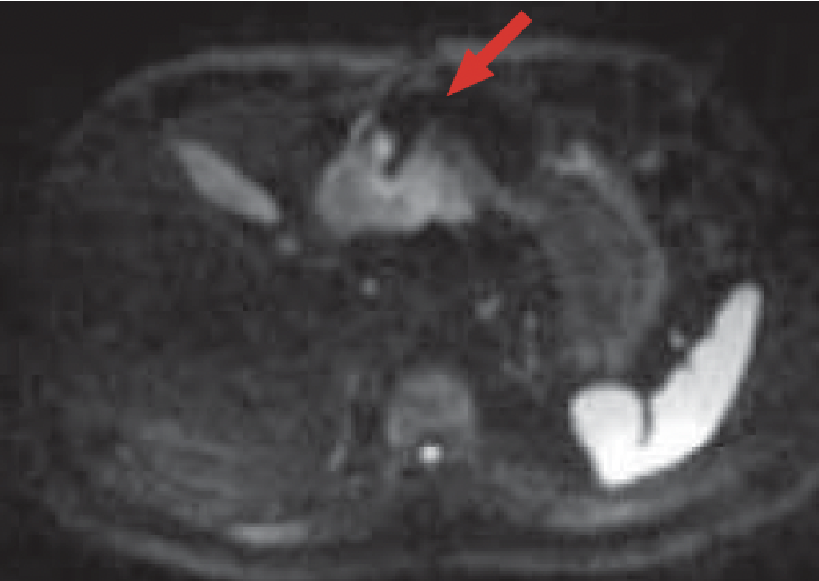
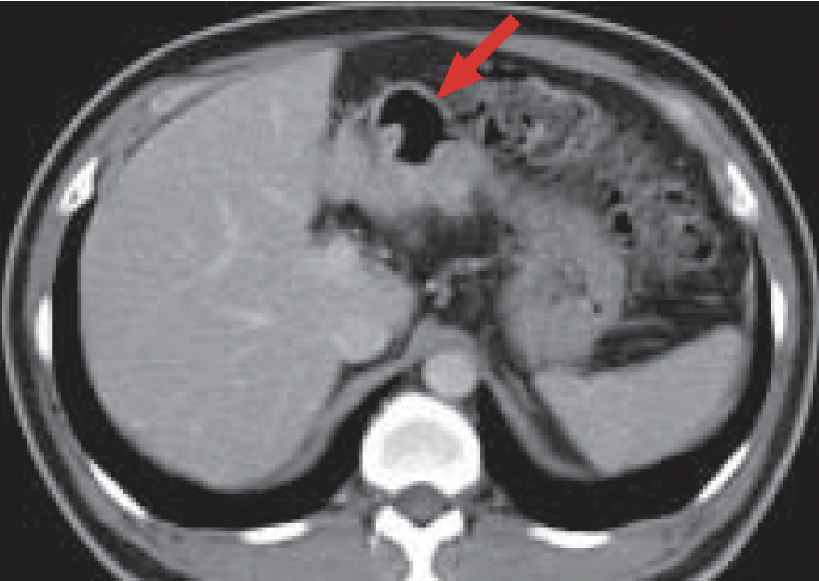
Diffusion-weighted imaging (q) showed an abnormally high signal in the gastric antrum (red arrow).
The contrast CT equilibrium phase (r) showed eccentric wall thickening (red arrow).
Type-2 advanced cancer was then confirmed by endoscopy.
Summary
The present patient was a special case, introduced to Dokkyo Medical University on the basis of a request for CT during angiography.
At the time of CT during angiography, there were few findings suggesting hepatic cirrhosis, but the arteriographic image and dynamic CT pattern were typical, and, in particular, corona-type dark staining was shown, suggesting HCC. However, when diffusion-weighted imaging was performed, the findings suggested gastric cancer, and a third nodule was found in the late phase of Gadoxetate disodium(Gd-EOB-DTPA) contrast MRI, enabling a preoperative diagnosis of hepatic metastasis. With Gadoxetate disodium(Gd-EOB-DTPA) contrast MRI, an overall assessment is made first, starting with observation in the hepatobiliary phase. However, if the non-tumor liver is found to be approximately normal, it should be recommended for priority to be given to assessment of the diffusion-weighted image. In addition, for detection of small mass lesions, the late phase of Gadoxetate disodium(Gd-EOB-DTPA) contrast MRI was considered to give the most readily comprehensible results, as it showed the same degree of dark staining in blood vessels and the hepatic parenchyma.
- * The case introduced is just one clinical case, so the results are not the same as for all cases.
- * Please refer to the Package Insert for the effects and indications, dosage and administration method, and warnings, contraindications, and other precautions with use.
