

A practical report of typical imaging of hepatocellular carcinoma (HCC): Diagnosis of HCC and its reliability
University of Tokyo Hospital
Institute of Medical Science Hospital, University of Tokyo
Dept. of Radiology:
Drs. Shigeru Kiryu (current position: Dean of Radiology, School of Medicine, International University of Health and Welfare), Yusuke Inoue (current affiliation: Dept. of Diagnostic Radiology, Kitasato University School of Medicine)
University of Tokyo Hospital:
Dept. of Radiology: Dr. Kuni Otomo (current position: President, International University of Health and Welfare)
Hepatobiliary and Pancreatic Surgery Division: Dr. Hiroshi Imamura (current affiliation: Dept. of Hepatobiliary Pancreatic Surgery, Juntendo University Hospital)
DATE : 2021
Diagnosis of HCC and its reliability

Patient’s background and objectives of magnetic resonance imaging (MRI)
Female, 70s.
During monitoring of progression of chronic hepatitis C, ultrasonography showed a hepatic mass, so the patient was admitted to hospital for thorough examination and treatment. Computed tomography (CT) was performed, and 1 week later MRI using Gadoxetate disodium(Gd-EOB-DTPA) was performed with the aim of qualitative diagnosis of the hepatic mass-type lesion.
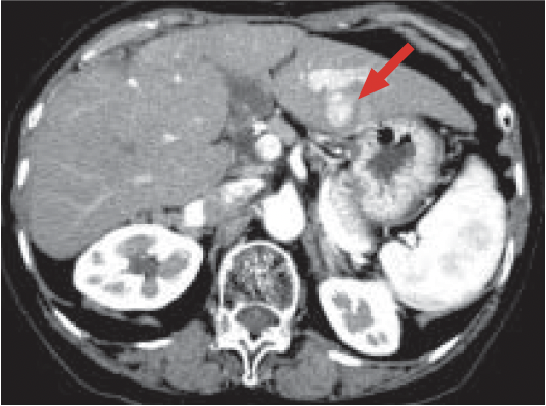
a) Arterial phase
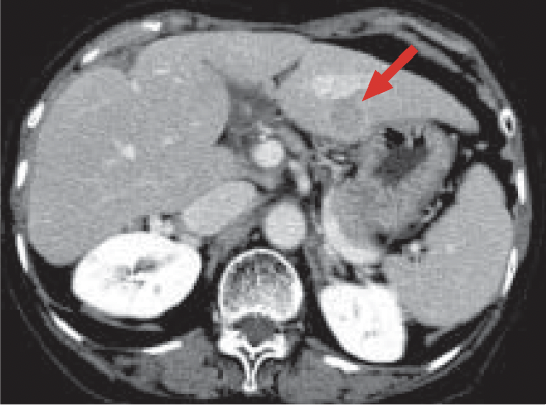
b) Portal phase
Multidetector CT
The arterial phase (a) showed a faintly dark-stained mass (arrow), 2 cm in diameter, in the lateral segment of the left lobe of the liver. Low absorption was found in the portal phase (b).
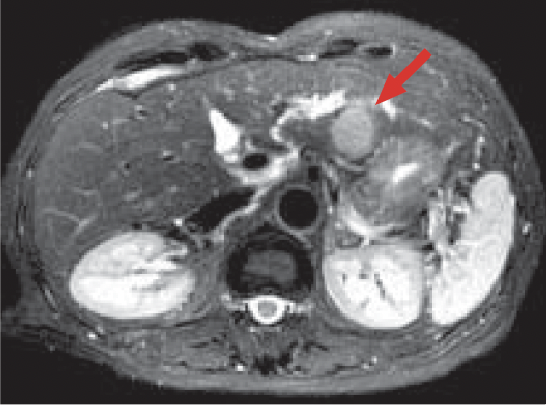
c) T2-weighted image

d) Pre-contrast, T1-weighted image
MRI
The mass (arrow) showed a high signal in the T2-weighed image (c), and a low signal in the T1-weighted image (d).
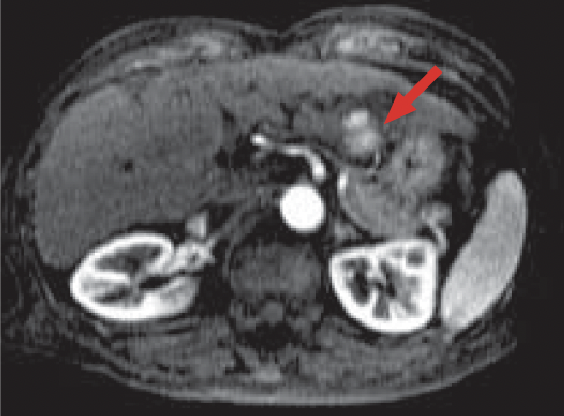
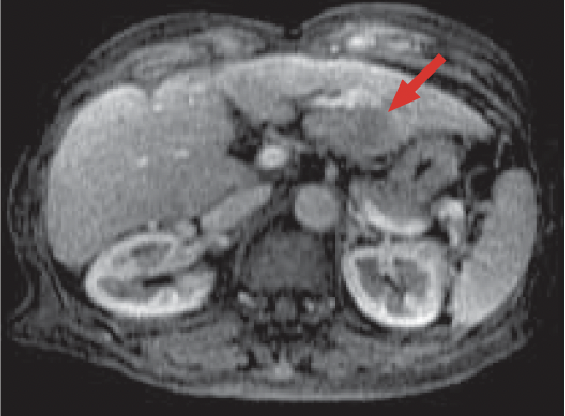
e) Arterial phase (20 s after administration)
f) 60 s after administration
g) 5 min after administration

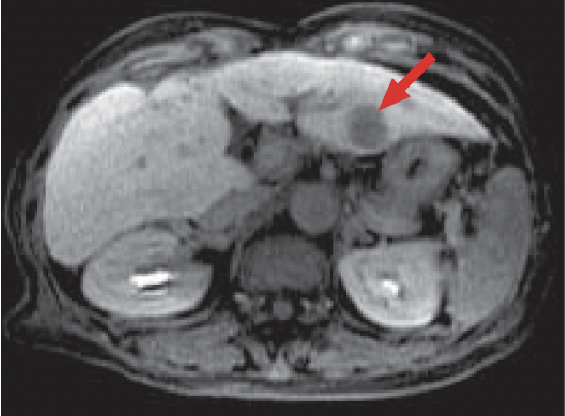
h) Hepatobiliary phase
Gadoxetate disodium(Gd-EOB-DTPA) contrast MRI
The mass (arrow) was shown as intensely dark-stained in the Gadoxetate disodium(Gd-EOB-DTPA) contrast MRI arterial phase (e). At 60 s after administration (f), the signal was even lower than in the surrounding hepatic parenchyma, and 5 minutes after administration (g) excretion of the contrast medium into the renal pelvis was found. In the hepatobiliary phase (h), 30 minutes after administration, dark staining was found in the surrounding hepatic parenchyma, but no distribution of the contrast agent to the mass was found, and there was favorable contrast with the surrounding hepatic parenchyma. In addition, excretion of the contrast agent into the biliary tract was found.
Impact of Gadoxetate disodium(Gd-EOB-DTPA) on diagnosis
Blood flow inside the mass was found to increase in the arterial phase, no uptake of Gadoxetate disodium(Gd-EOB-DTPA) by the mass was found in the hepatobiliary phase, and a definitive diagnosis of HCC was made on the basis of these findings. In addition, information about other segments was obtained.
Due to the low dose of the contrast agent, it is difficult to obtain appropriate images during the arterial phase. However, if flushing, an automatic injection device, etc., are used in the administration method, it is possible to achieve a favorable arterial phase. During the hepatobiliary phase, lesions can be investigated in detail using thin slices and a 3D gradient technique, and this technique is an improvement over MRI using superparamagnetic iron oxide contrast agents, in which the imaging is primarily 2D. The prolonged duration of the investigation can be problematic for studies using this contrast agent. However, if a dynamic study, such as post-contrast T2-weighted imaging and search for hepatic metastases, is omitted, one operational approach is to reduce the duration by administering the contrast agent before admitting the patient to the imaging theater .
Impact of Gadoxetate disodium(Gd-EOB-DTPA) on treatment
The most important issue for diagnosis of hepatic mass-type lesions is judgment as to whether monitoring of progression is sufficient, or resection or other treatment is needed, which broadly correlates with differentiation between benign and malignant masses. In the case of metastatic liver cancer, there is no inconsistency in it being a malignant mass at the time it is judged to be a mass. In the case of HCC, on the other hand, the multi-stage carcinogenesis process that it typically follows makes it rather difficult to decide upon the time when it should be diagnosed as an actual cancer requiring treatment. Diagnosis by CT, etc., is achieved by identifying hemodynamic changes inside the mass, these being changes in accessory properties. On the other hand, Gadoxetate disodium(Gd-EOB-DTPA) can be used to determine changes in hemodynamics, and at the same time to directly determine whether the mass is benign or malignant, that is, whether or not it is an aggregation of hepatocytes. This combination of capabilities is considered to be highly useful.
Precautions relating to administration
Administration to elderly patients
Elderly patients generally show depressed physiological function, so administration must be performed with care, and with sufficient monitoring of the patient’s condition.
- * The case introduced is just one clinical case, so the results are not the same as for all cases.
- * Please refer to the Package Insert for the effects and indications, dosage and administration method, and warnings, contraindications, and other precautions with use.
