

A case with which Gadoxetate disodium(Gd-EOB-DTPA) contrast MRI was used for detection of hepatocellular carcinoma (HCC): Practical report: Detection of micro-HCC
Juntendo University Nerima Hospital
Dept. of Radiology: Drs. Keigo Shimoji (currently Dept. of Radiology, Juntendo University Hospital), Shinsuke Kyogoku (currently Dept. of Radiology, Juntendo University Urayasu Hospital)
Dept. of Gastroenterology: Drs. Hironao Okubo, Shigehiro Kokubu, Akihisa Miyazaki
DATE : 2011
Detection of micro-HCC

Patient’s background and objectives of magnetic resonance imaging (MRI)
While the patient, a male in his 60s with chronic hepatitis C, was being monitored at a different hospital, computed tomography (CT) showed a nodule in the liver, and he was referred to the authors’ hospital, where dynamic CT was performed, and a hypervascular tumor was found in the liver. This was suspected of being HCC, so thorough examination, based on MRI using Gadoxetate disodium(Gd-EOB-DTPA), was performed in order to decide upon the approach to treatment. The interval between CT and MRI was approximately 14 days.
Slice section 1 (primary nodule)
(a) Pre-contrast
(b) Arterial phase
(c) Portal phase
MDCT
The pre-contrast image (a) showed a very faint low-absorption region, approximately 10 mm in diameter, in S6 of the liver (red arrow). The same area was dark-stained in the arterial phase (b; red arrow), and indistinct in the portal phase (c).
(d) T2-weighted image
(e) Pre-contrast T1-weighted image
MRI

(f) Arterial phase
(g) Late phase
(h) Hepatobiliary phase
Gadoxetate disodium(Gd-EOB-DTPA) contrast MRI
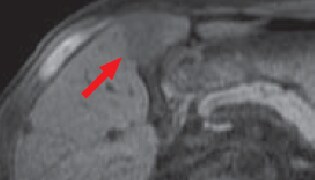
A nodule measuring approximately 31 × 23 mm was found in S4 of the liver (red arrow), with a faint high signal in the T2-weighted image (d), and a low signal in the T1-weighted image (e).
In the arterial phase after Gadoxetate disodium(Gd-EOB-DTPA) administration (f), the nodule (red arrow) showed a faint high signal, concentrated at the margins, whereas in the late phase the signal was lower than in the surrounding hepatic parenchyma.
In the hepatobiliary phase 20 minutes after administration (h), the nodule appeared as a low-signal region with distinct margins.
Slice section 2: Nodule diagnosis reliability increased by Gadoxetate disodium(Gd-EOB-DTPA) contrast MRI
(a) Pre-contrast
(b) Arterial phase

(c) Portal phase
MDCT
The pre-contrast image (a) showed a very faint low-absorption region, approximately 10 mm in diameter, in S6 of the liver (red arrow). The same area was dark-stained in the arterial phase (b; red arrow), and indistinct in the portal phase (c).
(d) T2-weighted image

(e) Pre-contrast T1-weighted image
MRI
(f) Arterial phase
(g) Late phase
(h) Hepatobiliary phase
Gadoxetate disodium(Gd-EOB-DTPA) contrast MRI
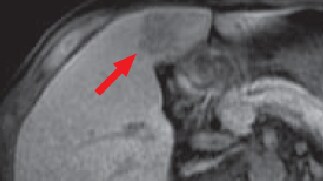
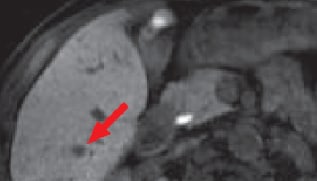
A nodule approximately 10 mm in diameter was found in S6 of the liver (red arrows), showing a high signal in the T2-weighted image (d) and a very faint low signal in the T1-weighted image (e).
The nodule (red arrow) was faintly dark-stained in the arterial phase after Gadoxetate disodium(Gd-EOB-DTPA) administration (f), and in the late phase it showed a lower signal than the surrounding hepatic parenchyma.
In the hepatobiliary phase 20 minutes after administration (h), the nodule appeared as a low-signal region with distinct margins.
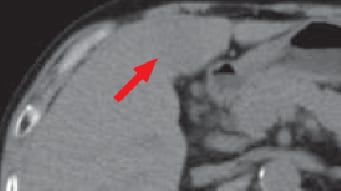
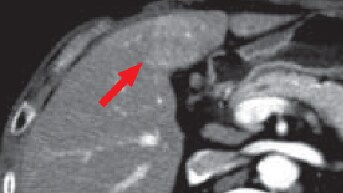
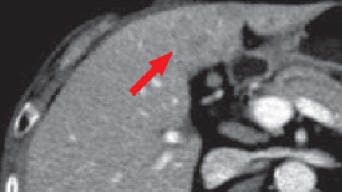
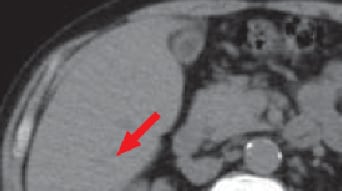
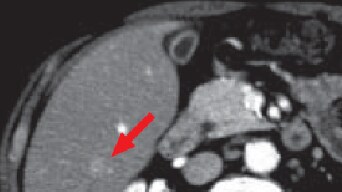
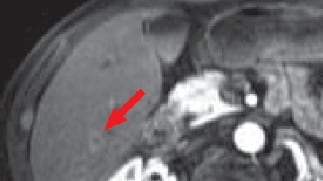
Slice section 3: Nodule not detected by dynamic CT, but detected by Gadoxetate disodium(Gd-EOB-DTPA) contrast MRI

(a) Pre-contrast
(b) Arterial phase
(c) Portal phase
MDCT
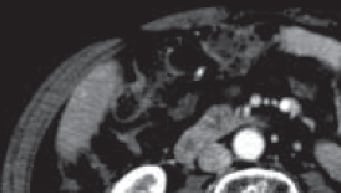
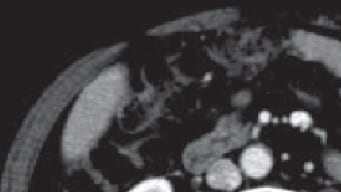
No region of abnormal absorption was found in the margin of S6 of the liver.

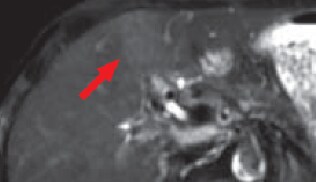
(d) T2-weighted image

(e) Pre-contrast T1-weighted image
MRI

(f) Arterial phase

(g) Late phase
(h) Hepatobiliary phase
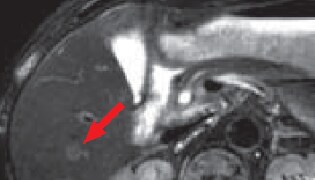
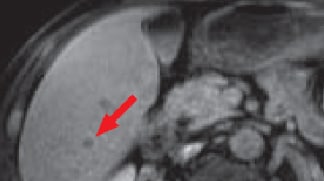
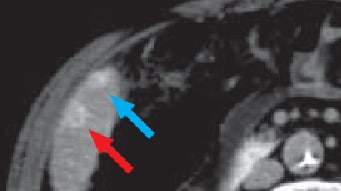
Gadoxetate disodium(Gd-EOB-DTPA) contrast MRI
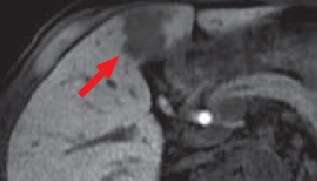
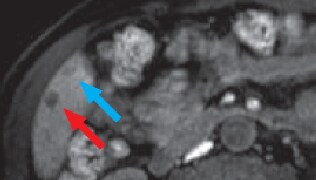
In S6 of the liver, the T2-weighted image (d) showed a slight high signal, and the T1-weighted image (e) showed a very faint low signal, so the existence of a nodule approximately 10 mm in diameter was suspected (red arrows).
The nodule in S6 of the liver was faintly dark-stained in the arterial phase after Gadoxetate disodium(Gd-EOB-DTPA) administration (f), and showed a mildly low signal in the late phase (g; red arrows).
In the hepatobiliary phase 20 minutes after administration (h), the same nodule appeared as a distinct low-signal region (red arrow), and the existence of a second nodule approximately 6 mm in diameter to its abdominal side was suspected (blue arrow).
(i) CT during hepatic angiography (CTHA)
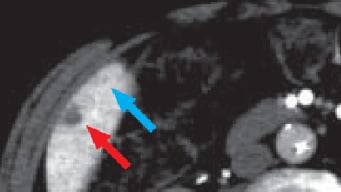
(j) CT during arterial portography (CTAP)
CT during angiography
The two nodules found in the hepatobiliary phase of Gadoxetate disodium(Gd-EOB-DTPA) contrast MRI (h; red and blue arrows) appeared dark-stained with CTHA (i), and as a contrast-deficient region with CTAP (j), these being performed at the same time.
Diagnostic findings and approaches to treatment
On the basis of the above findings, it was considered that the primary malignancy was a tumor in S4 of the liver, and that there were multiple hepatic metastases in the right lobe. The primary nodule in S4 of the liver showed faint vascularity, and could therefore have been HCC with low to moderate differentiation, or some other condition such as cholangiocellular carcinoma, or mixed liver cancer, and these had to be distinguished, so biopsy of this nodule was performed, and showed it to be moderately differentiated HCC. The treatment method selected was then chemotherapy with arterial injection.
Impact of Gadoxetate disodium(Gd-EOB-DTPA) on diagnosis
With this patient, the lesions that were indistinct after wash-out during dynamic CT, and the micro-lesions for which the images were indistinct were distinctly shown by Gadoxetate disodium(Gd-EOB-DTPA) contrast MRI, especially in the hepatobiliary phase, enabling highly reliable diagnosis of malignant tumors.
The numbers of lesions detected by Gadoxetate disodium(Gd-EOB-DTPA) contrast MRI and by CT during angiography (CTHA and CTAP) were consistent.
With Gadoxetate disodium(Gd-EOB-DTPA) contrast MRI, even in the case of micro-lesions, such as micro-HCC hepatic metastases, in the hepatobiliary phase favorable contrast was found between nodules and surrounding hepatic tissues, and the lesions were shown as distinct, low-signal regions, suggesting that Gadoxetate disodium(Gd-EOB-DTPA) contrast MRI has similar detection capacity to CT during angiography (CTHA and CTAP).
Impact of Gadoxetate disodium(Gd-EOB-DTPA) on treatment
The diagnoses made with the present patient by dynamic CT were a primary malignancy in S4 of the liver, and one hepatic metastasis in S6. The option of hepatectomy was considered initially, but Gadoxetate disodium(Gd-EOB-DTPA) contrast MRI was performed, and multiple hepatic metastases were clearly shown in the right lobe, so the treatment approach had to be switched to chemotherapy with arterial injection.
In conclusion, Gadoxetate disodium(Gd-EOB-DTPA) contrast MRI is considered to be an important technique for deciding upon the approach to treatment.
- *The case introduced is just one clinical case, so the results are not the same as for all cases.
- *Please refer to the Package Insert for the effects and indications, dosage and administration method, and warnings, contraindications, and other precautions with use.
